
- Messages
- 8,934
- Type of diabetes
- Type 1
- Treatment type
- Other
One of the great things about the Libre is your ability to test things like correction doses and whether they are right. But in tandem, you can also discover interesting things about the insulins you use...
This morning, by overnight level was higher than I wanted it to be, all be it flat (the Levemir doing a fabulous slow release job). When I awoke I checked my glucose level and it was too high, so I decided to correction dose of 1.5u, which according to my calcs should reduce my BG level by 4.5 mmol/l. As I was doing it from fasting, I thought it would be a good test.
Here's the result:
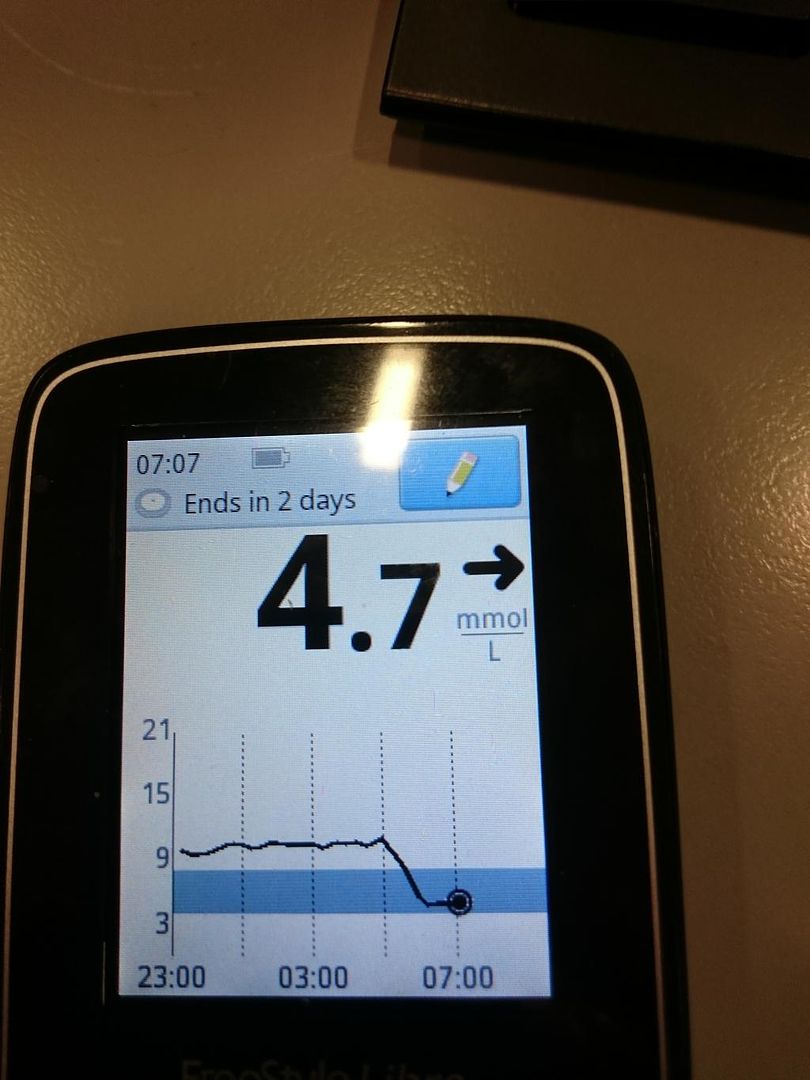
Overnight, the level ran at 9.4 (too high for my liking, but sometimes it happens - misadjustment for protein from the previous night). I tested at 4.45 and found this result.
The timeline is then as follows:
4.45am - Test - 9.4mmol/l
4.47am - Inject - 1.5u Novorapid into upper arm
5am approximately - Novorapid takes effect
7.07am - Test - 4.7mmol/l
I ate no food during this period, so this is a fasted test.
So what are my results from this test? The glucose drop was 4.7 mmol/l over the 2hr 20 mins period, confirming that my correction dose of 1u:3mmol wasn't far out. It's actually 1u:3.1mmol/l. That was the result I was looking for.
What I also learned is that in the injection site I used, the Novorapid kicks in within 15 minutes of injection. I know that other sites definitely take longer, so this was an interesting observation.
The second conclusion is that I get about two hours duration out of Novorapid in my system. We are told that the rapid insulins hang around for five or so hours, but the graph isn't suggesting this. From taking effect, it is clear that the Novorapid is no longer having a noticeable effect somewhere between 6.30am and 7am where the graph flattens out again (and more importantly, seems to stay flat).
So the conclusions I have taken from this little test were actually threefold.
This morning, by overnight level was higher than I wanted it to be, all be it flat (the Levemir doing a fabulous slow release job). When I awoke I checked my glucose level and it was too high, so I decided to correction dose of 1.5u, which according to my calcs should reduce my BG level by 4.5 mmol/l. As I was doing it from fasting, I thought it would be a good test.
Here's the result:
Overnight, the level ran at 9.4 (too high for my liking, but sometimes it happens - misadjustment for protein from the previous night). I tested at 4.45 and found this result.
The timeline is then as follows:
4.45am - Test - 9.4mmol/l
4.47am - Inject - 1.5u Novorapid into upper arm
5am approximately - Novorapid takes effect
7.07am - Test - 4.7mmol/l
I ate no food during this period, so this is a fasted test.
So what are my results from this test? The glucose drop was 4.7 mmol/l over the 2hr 20 mins period, confirming that my correction dose of 1u:3mmol wasn't far out. It's actually 1u:3.1mmol/l. That was the result I was looking for.
What I also learned is that in the injection site I used, the Novorapid kicks in within 15 minutes of injection. I know that other sites definitely take longer, so this was an interesting observation.
The second conclusion is that I get about two hours duration out of Novorapid in my system. We are told that the rapid insulins hang around for five or so hours, but the graph isn't suggesting this. From taking effect, it is clear that the Novorapid is no longer having a noticeable effect somewhere between 6.30am and 7am where the graph flattens out again (and more importantly, seems to stay flat).
So the conclusions I have taken from this little test were actually threefold.
- With no food in my system, my correction ratio is confirmed at 1u:3.1mmol/l
- NovoRapid can and does act within 15mins when fasted, in specific injection sites. Note the caveats.
- NovoRapid, when injected in these locations, endures for no more than 2.5 hours within my body.

