Hi, In something like February 2010, the results of a large scale study were published in the Lancet indicating that all cause morbidity was lowest in patients with a HbA1c level of 7.5% yet my medical team still recommend lower; does anyone have any more updated information than this? (My last result showed 59 (7.5) )
-
Guest - w'd love to know what you think about the forum! Take the 2026 Survey »
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
HbA1c and Morbidity
- Thread starter Taps18456
- Start Date
-
- Tags
- hba1c; morbidity
Indy51
Expert
Not sure if this relates to the specific paper you're referring to, but seems some of the studies recommending higher A1c's were confounded by aggressive lowering of BG by medications that had serious side effects:
http://www.phlaunt.com/diabetes/35169265.php
http://www.phlaunt.com/diabetes/35169265.php
BrianTheElder
Well-Known Member
- Messages
- 576
- Location
- Surrey, UK
- Type of diabetes
- Type 2
- Treatment type
- Diet only
- Dislikes
- Snide people
Thanks for that info, very interesting. Amazing what some of these researchers are prepared to do to their patients (victims).Not sure if this relates to the specific paper you're referring to, but seems some of the studies recommending higher A1c's were confounded by aggressive lowering of BG by medications that had serious side effects:
http://www.phlaunt.com/diabetes/35169265.php
That's interesting because I found myself in a conflict between my GP and endocrinologist - I've been living with diabetes for a long time and seemed to never get my A1cs in the 6 percent range - so I was referred to a specialist - the endo - and when I told him my doctor wanted tighter control he laughed and said just keep your A1cs in the 7s like you have been - he then told me that some of the studies being done in regard to tight control (this was about 5 years ago) had been cancelled because of the high mortality rate of the participants. I wish I had more information than that but that's all he told me - anyway - I don't get upset or panic if my Blood Sugars run high, I'll acto to get them down of course but some doctors seem to have fear instilled in their patients having them believe that if their BGs run high you will come down with nasty complications. I'm in my 51st year of living with Type 1 no serious complications yet .... maybe it has more to do with genetics than anything else - that's what my ophthalmologist keeps telling me.Not sure if this relates to the specific paper you're referring to, but seems some of the studies recommending higher A1c's were confounded by aggressive lowering of BG by medications that had serious side effects:
http://www.phlaunt.com/diabetes/35169265.php
Clivethedrive
Well-Known Member
That's interesting because I found myself in a conflict between my GP and endocrinologist - I've been living with diabetes for a long time and seemed to never get my A1cs in the 6 percent range - so I was referred to a specialist - the endo - and when I told him my doctor wanted tighter control he laughed and said just keep your A1cs in the 7s like you have been - he then told me that some of the studies being done in regard to tight control (this was about 5 years ago) had been cancelled because of the high mortality rate of the participants. I wish I had more information than that but that's all he told me - anyway - I don't get upset or panic if my Blood Sugars run high, I'll acto to get them down of course but some doctors seem to have fear instilled in their patients having them believe that if their BGs run high you will come down with nasty complications. I'm in my 51st year of living with Type 1 no serious complications yet .... maybe it has more to do with genetics than anything else - that's what my ophthalmologist keeps telling me.
Good evening @fletchweb, have a read of Dr Richard Bernsteins " Diabetes Solution 4 th ed.....i am following his reccomendations closely and so far so good,clive
Mep
Well-Known Member
- Messages
- 1,461
- Type of diabetes
- Treatment type
- Insulin
That's interesting because I found myself in a conflict between my GP and endocrinologist - I've been living with diabetes for a long time and seemed to never get my A1cs in the 6 percent range - so I was referred to a specialist - the endo - and when I told him my doctor wanted tighter control he laughed and said just keep your A1cs in the 7s like you have been - he then told me that some of the studies being done in regard to tight control (this was about 5 years ago) had been cancelled because of the high mortality rate of the participants. I wish I had more information than that but that's all he told me - anyway - I don't get upset or panic if my Blood Sugars run high, I'll acto to get them down of course but some doctors seem to have fear instilled in their patients having them believe that if their BGs run high you will come down with nasty complications. I'm in my 51st year of living with Type 1 no serious complications yet .... maybe it has more to do with genetics than anything else - that's what my ophthalmologist keeps telling me.
Yeh here they were pushing for tight control as well. Although it seems their parameters have changed as I used to be told I had to be under 7 at all times. With my hbA1c I get 6.8% a lot... I'm currently sitting at about 6.5% Although when I got over 7% I'd feel like I've failed. My highest hbA1c was 9.2% which my docs weren't impressed with. My endo now tells me I'm to aim for under 10 on my meter at all times and I should have at least 70% good numbers on my meter. At the moment I'm 80% in range. So I don't feel as bad these days with it. I have other issues affecting my blood sugar though so it's not easy keeping sugar levels in range all the time anyhow. All we can do is our best. Every time I see my endo now he just tells me I'm doing well and just wants to talk about all my other health conditions rather than my diabetes. He thinks diabetes is the least of my problems and told me I'm managing my levels well considering what I'm dealing with. Although I'm hard on myself and always feel I can do better.
he then told me that some of the studies being done in regard to tight control (this was about 5 years ago) had been cancelled because of the high mortality rate of the participants.
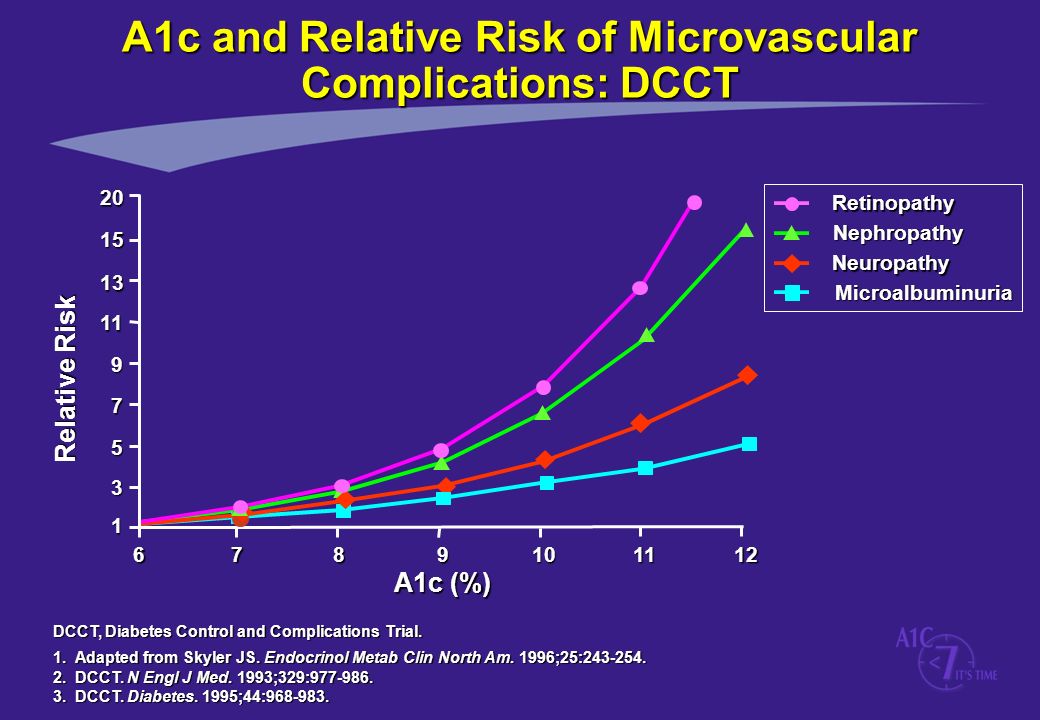
There are multiple different studies that often cause conflict in this particular area. The DCCT long term trial unequivocally demonstrated that there is an exponential relationship between increased risk of complications and Hba1C level in Type 1 diabetes, in that once you get to around 6.5%, for every percentage point above that you go, you multiply the risk of complications relative to a non-diabetic (as per the graph below).
The reference to studies being ended early refers to the ACCORD study that ended early due to unexpected higher levels of mortality in those treated intensively. It should be made very clear that this was a study primarily looking at CVD amongst Type 2s and as the Jenny Ruhl article states, used a drug in the intensive arm (primarily nearly 92% were taking Avandia, which is Rosiglitazone) which is no longer given to Type 2s due to the risk of heart attacks it induces. It is considered so dangerous that is was withdrawn from most global markets in 2010.
So in answer to both @fletchweb and @Taps18456 the studies that suggested that lowering Hba1C is dangerous for Type 2s has been massively discredited doe to the methods used, and aiming to get your Hba1C below 6.5% is very much the best thing to aim at, as it significantly reduces the risks of complications, and therefore death.
Clivethedrive
Well-Known Member
There are multiple different studies that often cause conflict in this particular area. The DCCT long term trial unequivocally demonstrated that there is an exponential relationship between increased risk of complications and Hba1C level in Type 1 diabetes, in that once you get to around 6.5%, for every percentage point above that you go, you multiply the risk of complications relative to a non-diabetic (as per the graph below).
The reference to studies being ended early refers to the ACCORD study that ended early due to unexpected higher levels of mortality in those treated intensively. It should be made very clear that this was a study primarily looking at CVD amongst Type 2s and as the Jenny Ruhl article states, used a drug in the intensive arm (primarily nearly 92% were taking Avandia, which is Rosiglitazone) which is no longer given to Type 2s due to the risk of heart attacks it induces. It is considered so dangerous that is was withdrawn from most global markets in 2010.
So in answer to both @fletchweb and @Taps18456 the studies that suggested that lowering Hba1C is dangerous for Type 2s has been massively discredited doe to the methods used, and aiming to get your Hba1C below 6.5% is very much the best thing to aim at, as it significantly reduces the risks of complications, and therefore death.
I entirely Agree as Dr R Bernsteins findinds show for every increase over 5.5% there are complications
But take heart it can be controlled as Dr bernstein and others are showing( Thank Goodness)
Very interesting as this relates to type 2 - I wonder if there are differences between type 1s and type 2s in regard to complications and A1C? More a curiosity than anything else. Let's face it the human body evolved to have a certain range of BG levels so it's common sense to try your best in achieving that. But statistically who gets the worse end of the deal in regard to complications - Type 1s or Type 2s - perhaps there is no difference - very intriguing ...There are multiple different studies that often cause conflict in this particular area. The DCCT long term trial unequivocally demonstrated that there is an exponential relationship between increased risk of complications and Hba1C level in Type 1 diabetes, in that once you get to around 6.5%, for every percentage point above that you go, you multiply the risk of complications relative to a non-diabetic (as per the graph below).
The reference to studies being ended early refers to the ACCORD study that ended early due to unexpected higher levels of mortality in those treated intensively. It should be made very clear that this was a study primarily looking at CVD amongst Type 2s and as the Jenny Ruhl article states, used a drug in the intensive arm (primarily nearly 92% were taking Avandia, which is Rosiglitazone) which is no longer given to Type 2s due to the risk of heart attacks it induces. It is considered so dangerous that is was withdrawn from most global markets in 2010.
So in answer to both @fletchweb and @Taps18456 the studies that suggested that lowering Hba1C is dangerous for Type 2s has been massively discredited doe to the methods used, and aiming to get your Hba1C below 6.5% is very much the best thing to aim at, as it significantly reduces the risks of complications, and therefore death.
Gee I must be a miracle then - In the 51 years I've been living with Type 1 I've only had one A1C in the 6s - most of the time I'm in the mid 7s. I'm in really good physical shape, always have been and very physically active - no complications. And I don't think I'm the only one - so I suspect there are additional variables that haven't been accounted for. Keep in mind I haven't read Bernsteins book yet so maybe he discusses this too. Either way I find it very interesting.I entirely Agree as Dr R Bernsteins findinds show for every increase over 5.5% there are complications
But take heart it can be controlled as Dr bernstein and others are showing( Thank Goodness)
