I am a type 1 diabetic I'm my 30s and have had the condition for 4 years. I am controlled by MDI and have used a Freestyle Libre since they came out.
I have had an HBA1C 5.6 / 38 for the last 3 years and it never varies.
I manage my condition by eating lower carb and as a result I tend not to get hypos.
During my twice yearly reviews, I normally get told that my HBA1C is too low and that I must be getting hypos, however with my Libre readings I can prove that I do not.
Surprisingly on my most recent review I was told by the DSN that I really need to raise my HBA1C not due to hypos as I don't get them, but because my HBA1C means I have a higher risk of heart disease than if it was in the 6 to 6.5 range.
I have been asked to go in and speak to my GP about it because the DSN couldn't explain why when I challenged.
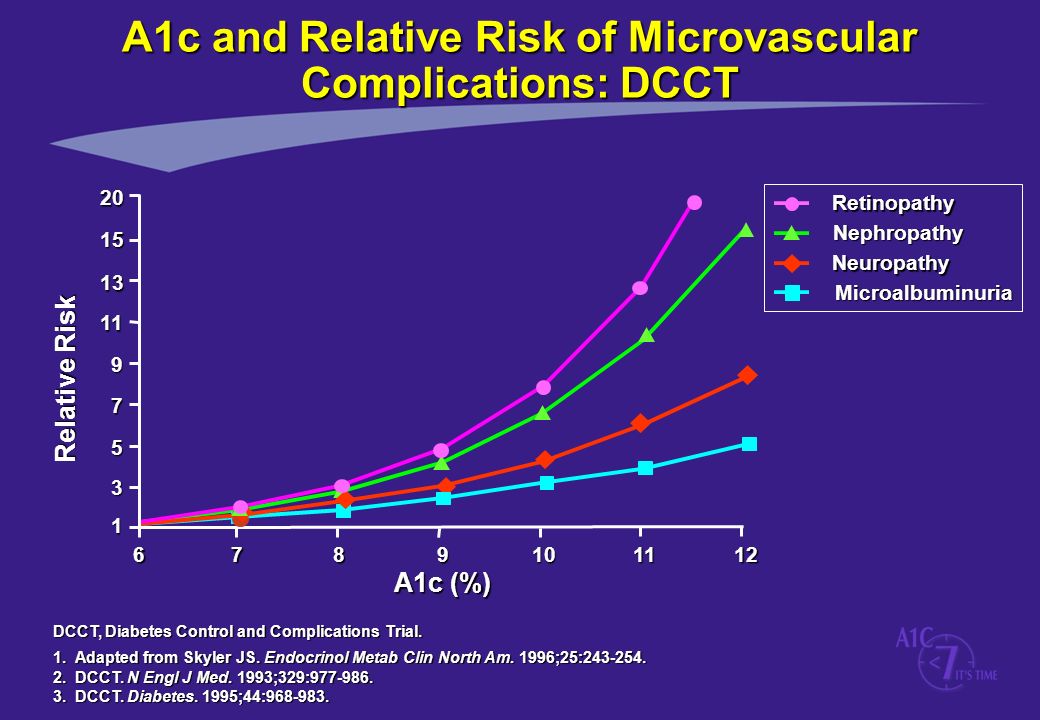
Based on the evidence I am familiar with there is a direct correlation between a increasing HBA1C and heart disease/ other complication risk. A quick Google search will support this.
Is anyone aware credible evidence that supports what the DSN has said?
I have had an HBA1C 5.6 / 38 for the last 3 years and it never varies.
I manage my condition by eating lower carb and as a result I tend not to get hypos.
During my twice yearly reviews, I normally get told that my HBA1C is too low and that I must be getting hypos, however with my Libre readings I can prove that I do not.
Surprisingly on my most recent review I was told by the DSN that I really need to raise my HBA1C not due to hypos as I don't get them, but because my HBA1C means I have a higher risk of heart disease than if it was in the 6 to 6.5 range.
I have been asked to go in and speak to my GP about it because the DSN couldn't explain why when I challenged.
Based on the evidence I am familiar with there is a direct correlation between a increasing HBA1C and heart disease/ other complication risk. A quick Google search will support this.
Is anyone aware credible evidence that supports what the DSN has said?