mrbondsbody
Member
- Messages
- 23
Hi mrbondsbody! I'm glad to see that several of the guys have mentioned MODY - it seems highly unlikely you are Type 2 - possible, but you do not have the main risk factors i.e. overweight, over 45, female with PCOS, of Asian origin and over 25 (obviously I don't know for sure you don't have this risk factor!). So, unlikely.
LADA would be the first thought - and the lack of antibodies do not actually rule that out (the presence of them would be a cause of diagnosis, but the absence doesn't rule it out). LADA is not hereditary although it is thought to have a genetic element, so your family history of diabetes would be largely a coincidence. I would say that although LADA is the most likely explanation, you do have the markers for the less common MODY - which is a whole set of different genetic forms of diabetes rather than a single condition. If you do have LADA, a VLCD will help with the most effective use of your remaining beta cells, but you will eventually progress to insulin, so you should test fairly frequently and make sure you insist on regular HbA1cs to make sure you don't end up very ill by failing to notice you have progressed beyond the point where you need insulin.
At your age i.e. an age where you have or might expect to one day have children, and with your family history of a non-progressing form of diabetes, the NHS is actually very sympathetic to funding MODY tests, because it is hereditary and you would want to know as soon as possible if you have passed the condition on to children (or might do one day). I think Exeter is the only place where tests for MODY are carried out, although that might have changed in the last few years.
Anyway, have a read of the Exeter MODY web site and if you think it's a possibility, ask your doctor about it - but be prepared that they'll know nothing about MODY and you might need to contact Exeter yourself to see what your options are for testing.
Nothing wrong with low-carb though whichever type of diabetes you have!
Smidge
Yes, that's the point, isn't it. Until and unless your blood sugars rise, only your diet will change, no?
I still wouldn't do it, though. It's VLCHF that is keeping your bloods at a safe normal level. That is great. And I don't see how reintroducing you to non-ketogenic carb levels and waiting to see if you develop v high BG and dangerous levels of ketones can possibly be responsible. If there's a good reason, It's a mystery to me.
If your BG eventually rises, then it will be clear that you do need insulin, ie that you're type 1. That you can catch by testing, and I think that's what you should do.
I don't know what to suggest about tests. Is it GAD you got a negative result on? Phoenix is your best guide here.
So just keep monitoring your BG and, if it begins to rise steadily, your ketones too. It's high BG though - over ? 11 ? - that will be your tripwire. And if your BG rises seriously, you'll be asking for insulin, won't you?
Thank goodness, with diabetes we can do a lot ourselves.
Lucy
I'm also confused as to why your doc wants to reintroduce carbs and check for ketones. Have you had an HBa1c test done? The best bet would be her suggestion to do a C-peptide test. Until then LADA, MODY or T2 are all options. Or even straight T1.
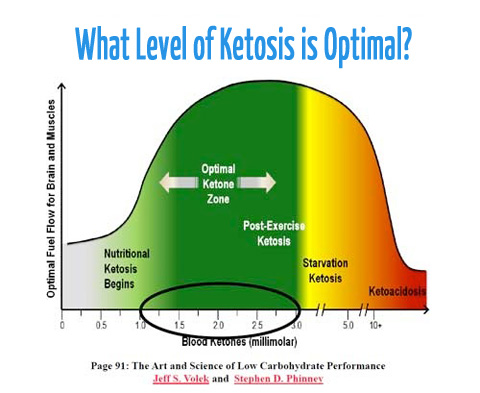
The only thing I'm slightly concerned by is that your 2.5 ketone level is on the higher side for nutritional ketosis. That's a blood level and not a urine level right? Have the ketones be tested regularly or just the once, at your first presentation to the doc?
http://emedicine.medscape.com/article/117739-workup#a0756Islet-cell (IA2), anti-GAD65, and anti-insulin autoantibodies can be present in early type 1 but not type 2 DM. Measurements of IA2 autoantibodies within 6 months of diagnosis can help differentiate between type 1 and type 2 DM. These titers decrease after 6 months. Anti-GAD65 antibodies can be present at diagnosis of type 1 DM and are persistently positive over time
Only about two models of monitor work with blood ketone strips (obtained separately). One is the Glucomen LX. Is the other the One Touch Verio Pro??I can't seem to get my monitor to work with ketones.
But isn't up to 3.0 blood ketones okay? Ketosis ( nutrititional), but not DKA? Ask @robert72 who has a great diagramyep that's blood level, 1.5 hs after breakfast at the hospital. I can't seem to get my monitor to work with ketones.
I'll get the c-peptide test and mody done as soon as I go back to the hospital.
thx for all your help
The Abbott Freestyle Optium Neo is anotherOnly about two models of monitor work with blood ketone strips (obtained separately). One is the Glucomen LX. Is the other the One Touch Verio Pro??
Hi mrbondsbody! I'm glad to see that several of the guys have mentioned MODY - it seems highly unlikely you are Type 2 - possible, but you do not have the main risk factors i.e. overweight, over 45, female with PCOS, of Asian origin and over 25 (obviously I don't know for sure you don't have this risk factor!). So, unlikely.
LADA would be the first thought - and the lack of antibodies do not actually rule that out (the presence of them would be a cause of diagnosis, but the absence doesn't rule it out). LADA is not hereditary although it is thought to have a genetic element, so your family history of diabetes would be largely a coincidence. I would say that although LADA is the most likely explanation, you do have the markers for the less common MODY - which is a whole set of different genetic forms of diabetes rather than a single condition. If you do have LADA, a VLCD will help with the most effective use of your remaining beta cells, but you will eventually progress to insulin, so you should test fairly frequently and make sure you insist on regular HbA1cs to make sure you don't end up very ill by failing to notice you have progressed beyond the point where you need insulin.
At your age i.e. an age where you have or might expect to one day have children, and with your family history of a non-progressing form of diabetes, the NHS is actually very sympathetic to funding MODY tests, because it is hereditary and you would want to know as soon as possible if you have passed the condition on to children (or might do one day). I think Exeter is the only place where tests for MODY are carried out, although that might have changed in the last few years.
Anyway, have a read of the Exeter MODY web site and if you think it's a possibility, ask your doctor about it - but be prepared that they'll know nothing about MODY and you might need to contact Exeter yourself to see what your options are for testing.
Nothing wrong with low-carb though whichever type of diabetes you have!
Smidge
http://www.bpac.org.nz/BT/2013/November/lipid-testing.aspxTriglyceride levels are increased for six to eight hours after a standard meal.1, 3 If a patient has consumed a very high fat content meal prior to testing, or if they have slow lipid particle clearance after food (post-prandial dyslipidaemia), triglyceride levels could be increased more than the estimated 0.3 mmol/L variance, and misrepresent clinical significance

")