Okay you guys!
I believe that I found the answer to this phenomenon and it is the circadian rhythm or, otherwise called, the biological clock.
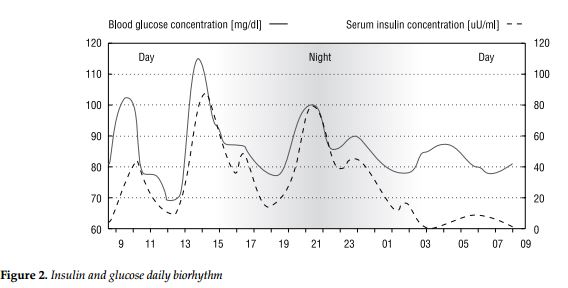
According to the circadian rhythm, most of the body’s major physiological functions fluctuate with the time of day. Examples include body temperature, hormone secretion, urine production, blood circulation, metabolism, and even the growth of hair. These fluctuations usually go through a peak and a trough that coincide with particular times of day. For example, human body temperature is always lowest at night.
As diabetics we all know the “dawn phenomenon” which is the hormone cortisol peak secretion and occurs just before a person wakes up, so that this hormone’s level is highest when the person gets out of bed, thus contributing to the general activation of the body.
This is where most of us see a blood sugar rise.
Alright, so we know that. We have established that.
Here is the tricky part now.
The circadian cycle is divided into two sub-cycles of about 12 hours each.
The
first and longest period of sleepiness occurs around the time that you are used to going to bed and is deepest between 3:00 AM and 6:00 AM. This is the time of day when your metabolism and body temperature are at their lowest. The body slows down, the hormones calm down as well and this is why most of us who check regularly during the night (myself included) may have noticed a dip in our blood glucose in between 03:00 – 05:00 0r 06:00. After this, the dawn phenomenon kicks in.
The second daily period of sleepiness occurs 12 hours later, between 2:00 PM and 4:00 PM. This period is shorter than the one that occurs at night, but we all know it well—it’s the mid-afternoon slump.You may have noticed that your body becomes more receptive towards insulin during these hours. I know mine does.
However, around 16:00 – 17:00 the biological clock makes us alert again.
Hormones come back into play therefore, we experience a phenomenon which is somewhat similar to the dawn phenomenon.
It is a little bit like the dawn phenomenon only that it occurs in the afternoon.
And this explains why some people, myself included, see an unexplained blood sugar rise in between 16:00 to 18:00
Now, if in this scheme, we include our insulin peaking hours, we get our pattern.
I will use myself as an example. In my case, I inject my morning Levemir at 07:00 am.
This injection peaks at 8-10 hours therefore, my basal insulin’s peak is in between 15:00 -17:00 pm.
My Lunchtime Novorapid is at 13:00.
This injection peaks at 1.5-2.5 hrs therefore, my bolus peak is in between 14:30 – 15:30.
It is very logical, in my mind at least, that with 2 insulins (basal and bolus) peaking at around the same time) plus a circadian circle that is more receptive during these hours, that I will see a drop in my blood glucose.
And, at 17:00, when both my basal insulin stabilizes and my Novorapid tails off, the body hormones come into play and I see a rise from 17:00 up until 18:00.
Fascinating, aint it?
In relation to food, what I have noticed is that, indeed, when I add butter or oil (or any other fat) at lunch, my food (which is already very low GI) delays even more. Therefore, my blood sugar drop in between 14:00-16:00 will be even bigger.
I noticed that if there is fat in my lunch the drop in between these hours can be even upto 4 mmols.
Without fat, and a bit of fruit (to change my meal to a medium GI) the blood glucose drop is about 1.5-2 mmols. In both cases, there is no activity involved during these hours.
Now, here is the question: How do I address the post-lunch drop and then the rise?
Well, unless I get a pump, I cannot. Because I am not still very confident to split Novorapid doses.
I discussed the matter with my doctor who suggested that, for the time being (and until I get a pump) I will have to live with it (just like I have to live with the dawn phenomenon and correct with my breakfast.)
I will try to see if a little bit of exercise in between 16:00-18:00 could push this rise downwards.
My doctor’s approach is not the ideal approach but, if I manage to get my levels within target for the rest of the 24 hrs then, maybe I can live with a small spike during the day.
I hope that you found this post useful.
Regards
Josephine.
P.S. There are more interesting things about the circadian rhythm and how our body becomes more responsive or more resistant to insulin during the 24 hours. I intend to post more about it and I hope that you will find it useful!
View attachment 17099
")


") Not sure how maintainable it is though....
Not sure how maintainable it is though.... 
