Hi, whilst Ken has been writing his summary, I've been drawing graphs.
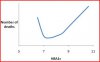
Using the limited figures given, a graph of the deaths in the lancet study would look a bit like this
(it really is only to give a idea its not accurate)
There are several possibilities as to why this higher rate of death at lower rates might be.
For example in the lancet study. (and I'm sure there are lots of other interpretations)
1) people who are very ill and particularly with end stage renal problems have a lower HbA1c, this could skew the data.(it was death from all causes).
2) insulin is prescribed quite later or when other methods have 'failed' in type 2 diabetes in the UK.
a)it might be a case of too little too late, the insulin reduces the HbA1c but sometimes well after the complications have developed
b) it could mean that the medication itself was the problem(as Ian) suggests
3) The quality of data used in the study might itself be a problem (doctors records)
Just to show how confusing the data is (and why you can't make a blanket interpretation)
This slide shows some of the data from the ACCORD study. In this one there was a higher mortality rate in the intensive arm... this is the one medicated to achieve a lower HbA1c, but even in this arm there were fewer deaths than in other studies. Also in this intensive arm there was a reduced risk of non fatal complications.
Moral: people need to have targets based upon their indivdual circumstances. For some low levels will not be appropriate.
There is a line of thought that diabetes (particularly T1, with DAFNE) can be controlled by medication, while eating normally. That is where Hana & I & others take issue. A reduced carb diet will not have such adverse effects. Hana's husband has been T1 for many years
I really don't know what grounds you have for this statement. Using injected insulin in a way that attempts to mimick the natural functions of endogenous insulin seems to me to be a very sensible practice, where is the evidence for adverse effects?